




Lupine Publishers Group
Lupine Publishers
ISSN: 2638-5945
Case Report(ISSN: 2638-5945) 
Acute Erythroblastic Leukemia Revealed by Dermatological Manifestations Volume 1 - Issue 2
Received: February 17, 2018; Published: February 21, 2018
*Corresponding author: Kaoutar Moustaide, University Hospital Hassan II, Route sidi Hrazem Fes, North Africa
DOI: 10.32474/OAJOM.2018.01.000106
Also view in:






Abstract
Acute erythroblastic leukemia is characterized by the proliferation of a predominant erythrocyte population on other lineages. Cutaneous manifestations remain rare and misleading, making the diagnosis of difficult to suspect as first-line. Here, we report an unusual and rare case of acute leukemia in a 24 year old male with gingival hypertrophy and dermatological manifestations. This case emphasizes that dentist and dermatologist should be well acquainted with these manifestations of systemic diseases.
Case Report
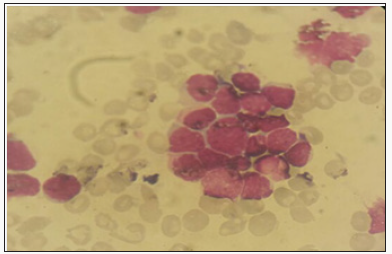
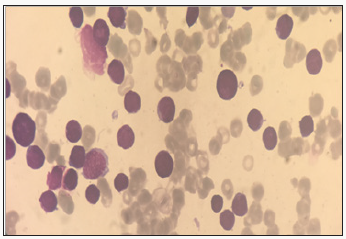
We report the case of 24 years old patient, with no significant pathological history, who had a rash for 10 days in a context of fever and very bad general condition. At admission the patient was febrile, tachycardic and dyspneic. Physical examination revealed erythemato-purplished papulo-nodules on the face, trunk, limbs and a gingival hyperplasia. The oral state was deplorable. Bilateral cervical lymphadenopathy was also found without the patosplenomegaly (Figures 1-3). The biological assessment showed a CRP of 150 and a pancytopenia with a Hbat 7.5g / dl, normal VGM and CCMH, a deep thrombocytopeniaat 85000 / l, leukocytesat 1500 / l. The blood smear showed 35% of circulating blasts and 22% of erythroblasts (Figure 4).
Figure 1: Clinical Manifestations of AML.

Figure 2: Clinical Manifestations of AML.
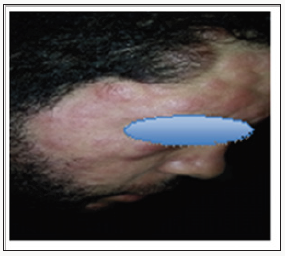
Figure 3: Clinical Manifestations of AML.
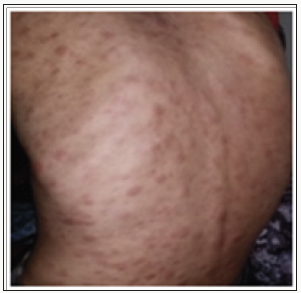
Figure 4: Blood smear showing 35% of circulating blasts.
The medullo gram showed a hyper-cellular marrow with a rate of myeloblasts greater than 45% compared to all non-erythroblastic elements and erythroblastic hyperplasia estimated at more than 65%; with signs of dyserythropoiesis suggestive of the diagnosis of erythroleukemia (Figure 5). Blood immune phenol typing was positive for CD13, CD33, MPO and Glycophotin A. The evolution was unfavourable; the patient died due to massive alveolarhemorrhage.
Figure 5: Hyper cellular marrow infiltrated by a blastic contingent estimated at 45%.
Discussion
Acute erythroblastic leukemia is characterized by the proliferation of a pre dominantery throcyte population on other lineages. There are two types: Erythroleukemia: defined by the presence in the bone marrow of more than 50% of the erythroid precursors of all the medullary cells, and more than 20% of myeloblasts of the whole non-erythrocytemedullary cells - Pure erythroid leukemia: it presents a neoplastic proliferation made of more than 80% of erythrocyte cells without obvious presence of the myeloblastic contingent [1]. It is usually manifested by signs of bone marrow failure and cytopenia [2,3], skin involvement remains rare, varied and disorienting the diagnosis; they are found mainly in Acute myelovlastic leukemia [4,5]. Cutaneous manifestations during leukemia are infrequent and varied. They designate all the cutaneouslesions related to the haematological malignancy directly or indirectly following their treatment; we essentially distinguish.
The specific dermatological lesions which can reveal hematological diseases [4], are mainly represented by leukaemides (leukaemia cutis), which are red brown to purple dermal papules, plaques or nodules. Granulocyticsarcom as an extra-medullary tumour masses, ulcerated plaques and gingival hypertrophy [5]. The infectious dermatoses secondary to the biological disturbances accompanying the malignan themopathy and their treatments. The occurrence of specific cutaneouslesions in leukemia is synonymous with a major aggravation of the prognosis (with for example a survival twice as short if there is a specific cutaneous involvement); this seriousness make some authors propose different treatments with a medium-long stay hospitalization[6-8].
In our case, acute myelonlastic leukemia 6 (AML 6 ) was revealed by diffuse leukemias resulting from the infiltration and proliferation of malignantha ematological cells (blasts) in the skin and by gingival hyperplasia secondary to mucosal infiltration [5]. The clinical presentation of acute leukemia including AML6 in the form of ulcer ativenecroticgingivitis in the foreground, is a rare form to be remembered, mentioned in all courses of medicine and dentistry, stipulating that Gingival involvement is a classic feature of leukemia [6] The frequent association of skin cancers with haematological malignancies is also highlighted in several publications [5].
Conclusion
The cutaneous localizations are among the rarest extreme dullary lesions of acute myeloid leukaemia’s (AML) not exceeding 1%. They are generally considered as factors of worse prognosis. Their cytogenetic or mutational specificities remain un established to date.
References
- Imane Tlamçani, Salma Benjelloun, Ghita Yahyaoui, Moncef Hassani Amrani (2014) Leucémie aigue érythroblastique: à propos de sept observations. The Pan African Medical Journal Published: 18/05/2014.
- Killick S, Matutes E (2002) Acute Erythroid leukaemias. Atlas Genet Cytogenet Oncol Haematol.
- Killick S, Matutes E, Powles RL, Min T, Treleaven JG, et al. (2014) La leuc émie aigue érythroïde (M6): résultat de la transplantation de moelle osseuse. Leukemia and Lymphoma.
- Blessis D, Frances C, Grillot J (2009) manifestations dermatologiques des maldies du système hématologique et oncologie dermatologique. Dermatologie et medicine, Springer Verlag, France.
- H Bay BayLes (2011) manifestations cutanées au cours des hémopathies malignes, EM consulte.
- Arnaud Lafon, Thomas Belangeon, Victorin Ahossi, Patrick Larras, Daniel Perri, et al. (2010) Leucémie aiguë myéloïde : le tableau clinique est parfois trompeur. Service d’Odontologie, MBCB Journal.
- Dan Lipsker, PeggyBoeckler (2007) Manifestations cutanées associées aux paraproteines,mechanism e des atteintes cutanées, La Presse Médicale 36(8): 1135-1140.
- Namba Y, Koizumi H, Nakamura H, Taromi T, Sawada K, et al. (1999) Specific cutaneous lesions of the scalp in myodysplastic syndrome with deletion of 20q. J Dermatol 26(4): 220-224.


-

Mark E Smith
Bio chemistry
University of Texas Medical Branch, USA -

Lawrence A Presley
Department of Criminal Justice
Liberty University, USA -

Thomas W Miller
Department of Psychiatry
University of Kentucky, USA -

Gjumrakch Aliev
Department of Medicine
Gally International Biomedical Research & Consulting LLC, USA -

Christopher Bryant
Department of Urbanisation and Agricultural
Montreal university, USA -

Robert William Frare
Oral & Maxillofacial Pathology
New York University, USA -

Rudolph Modesto Navari
Gastroenterology and Hepatology
University of Alabama, UK -

Andrew Hague
Department of Medicine
Universities of Bradford, UK -

George Gregory Buttigieg
Maltese College of Obstetrics and Gynaecology, Europe -

Chen-Hsiung Yeh
Oncology
Circulogene Theranostics, England -
.png)
Emilio Bucio-Carrillo
Radiation Chemistry
National University of Mexico, USA -
.jpg)
Casey J Grenier
Analytical Chemistry
Wentworth Institute of Technology, USA -

Hany Atalah
Minimally Invasive Surgery
Mercer University school of Medicine, USA -

Abu-Hussein Muhamad
Pediatric Dentistry
University of Athens , Greece
